
An Overview of Recent Findings
The United States continues to be in the grasp of an opioid epidemic. According to research done by the Rockefeller Institute of Government, drug death rates increased in almost every state between 2015 and 2016 — and those numbers continue to rise. The damage from opioid abuse is not limited to individual users, but has ripple effects that impact families, communities, and governments. Policymakers and activists are grappling with how to best address the problem, but are often stymied by budget constraints and a lack of evidence as to what actually works. Recent research, however, has found that legal access to marijuana may be a potential tool for addressing the opioid crisis.
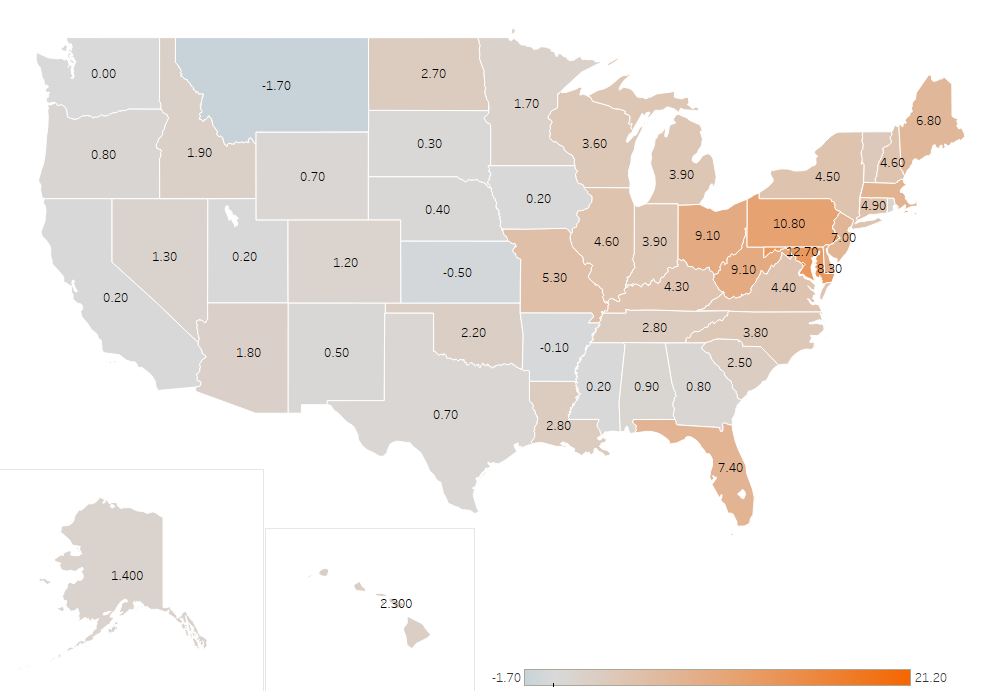
Increase in Drug Death Rates by State and District of Columbia, 2015-16
| State | 2015 | 2016 | Change |
| District of Columbia | 19.3 | 40.5 | 21.2 |
| Maryland | 22.0 | 34.7 | 12.7 |
| Pennsylvania | 26.4 | 37.2 | 10.8 |
| Ohio | 29.4 | 38.5 | 9.1 |
| West Virginia | 40.7 | 49.8 | 9.1 |
| Delaware | 22.0 | 30.3 | 8.3 |
| Massachusetts | 27.2 | 34.9 | 7.7 |
| Florida | 16.7 | 24.1 | 7.4 |
| New Jersey | 16.8 | 23.8 | 7.0 |
| Maine | 20.9 | 27.7 | 6.8 |
| Missouri | 18.0 | 23.3 | 5.3 |
| Connecticut | 23.0 | 27.9 | 4.9 |
| New Hampshire | 32.5 | 37.1 | 4.6 |
| Illinois | 14.6 | 19.2 | 4.6 |
| New York | 15.2 | 19.7 | 4.5 |
| Virginia | 12.8 | 17.2 | 4.4 |
| Kentucky | 30.1 | 34.4 | 4.3 |
| Indiana | 19.8 | 23.7 | 3.9 |
| Michigan | 23.3 | 27.2 | 3.9 |
| North Carolina | 16.3 | 20.1 | 3.8 |
| Wisconsin | 15.5 | 19.1 | 3.6 |
| Vermont | 17.7 | 21.0 | 3.3 |
| Louisiana | 19.3 | 22.1 | 2.8 |
| Tennessee | 23.4 | 26.2 | 2.8 |
| North Dakota | 8.6 | 11.3 | 2.7 |
| South Carolina | 16.2 | 18.7 | 2.5 |
| Hawaii | 12.2 | 14.5 | 2.3 |
| Oklahoma | 19.2 | 21.4 | 2.2 |
| Idaho | 13.5 | 15.4 | 1.9 |
| Arizona | 19.8 | 21.6 | 1.8 |
| Minnesota | 11.9 | 13.6 | 1.7 |
| Alaska | 17.2 | 18.6 | 1.4 |
| Nevada | 21.8 | 23.1 | 1.3 |
| Colorado | 16.4 | 17.6 | 1.2 |
| Rhode Island | 30.1 | 31.2 | 1.1 |
| Alabama | 16.7 | 17.6 | 0.9 |
| Oregon | 15.1 | 15.9 | 0.8 |
| Georgia | 13.4 | 14.2 | 0.8 |
| Wyoming | 16.9 | 17.6 | 0.7 |
| Texas | 9.9 | 10.6 | 0.7 |
| New Mexico | 24.7 | 25.2 | 0.5 |
| Nebraska | 7.3 | 7.7 | 0.4 |
| South Dakota | 8.4 | 8.7 | 0.3 |
| Iowa | 10.6 | 10.8 | 0.2 |
| California | 12.8 | 13.0 | 0.2 |
| Mississippi | 12.3 | 12.5 | 0.2 |
| Utah | 22.3 | 22.5 | 0.2 |
| Washington | 16.6 | 16.6 | 0.0 |
| Arkansas | 14.3 | 14.2 | -0.1 |
| Kansas | 12.0 | 11.5 | -0.5 |
| Montana | 14.7 | 13.0 | -1.7 |
Source: “Opioid Deaths Continue to Surge in New York State,” citing data from the Centers for Disease Control and Prevention
In April 2018, two new studies in JAMA Internal Medicine looked at the impact of legalized medical marijuana on the rate of opioid prescriptions. One study examines if the presence of state medical and recreational marijuana laws have an impact on the prescription rate of opioids for Medicaid enrollees. The over-prescription of opioids has been cited as a contributing factor to the current epidemic. If marijuana is a legal alternative for pain management, will opioids be less likely to be recommended?
The authors use State Drug Utilization Data from the Centers for Medicare & Medicaid Services (CMS) from the first quarter of 2011 to the second quarter of 2016. During this time frame, eight states (Connecticut, Delaware, Illinois, Maryland, Massachusetts, Minnesota, New Hampshire, and New York) implemented marijuana laws, while four states (Alaska, Colorado, Oregon, and Washington) that already had medical marijuana programs implemented recreational marijuana laws. Medicaid spending on prescription opioids was also examined.
A study in the March 2018 issue of the Journal of Health Economics found a link between states that have medical marijuana dispensaries and a decrease in opioid mortality rates.
The researchers found that the implementation of state medical and recreational marijuana laws was associated with a lower prescription rate of Medicaid-covered opioids — a 5.88 percent lower rate of Medicaid-covered opioids in states that had implemented medical marijuana legislation and an additional 6.38 percent lower opioid prescription rate in states that also implemented recreational marijuana use. Recreational marijuana laws also were found to be associated with 9.78 percent lower Medicaid spending on prescription opioids, an annual savings of $1,815 Medicaid spending per 1,000 enrollees.
The second study by University at Georgia researchers focuses on the impact of state medical marijuana laws from 2010 to 2015 on the prescription of opioids under Medicare Part D, relying on data from the CMS. Particular attention was paid to the distinction, if any, between states that allow marijuana to be purchased at a dispensary versus states that only permit home cultivation. The impact of recreational marijuana laws was not examined. Overall, patients in states with medical marijuana laws filled fewer daily doses of opioids. The results found a 14.4 percent reduction in the use of opioids by Medicare patients in states with access to a medical marijuana dispensary, and a 6.9 percent opioid use reduction in states that only permitted home cultivation of medical marijuana.
| Access to Medical Marijuana | Reduction in Use of Opioids by Medicaid Patients |
| States with access to a medical marijuana dispensary | 14.4% |
| States that permit only home cultivation of marijuana | 6.9% |
While there are limitations of both these studies that caution against overstating the applicability of findings, they are the latest in a research trend that has found positive correlations between legal access to marijuana and a decrease in opioid-related use and/or death. A 2014 JAMA Internal Medicine article showed that medical marijuana laws are associated with lower state-level opioid mortality rates. A 2017 Drug and Alcohol Dependence study demonstrated that hospitalizations associated with opioid pain relievers were reduced in states that had medical marijuana policies enacted. A study in the March 2018 issue of the Journal of Health Economics found a link between states that have medical marijuana dispensaries and a decrease in opioid mortality rates. A 2016 article in The Journal of Pain found patients that suffered with chronic pain and used medical marijuana were 64 percent less likely to report the use of opioids. It is important to note, however, that not all recent research findings have been positive — earlier this year, research in The American Journal of Psychiatry found that marijuana use actually increases the risk of an opioid-use disorder.
Not all recent research findings have been positive — earlier this year, research in The American Journal of Psychiatry found that marijuana use actually increases the risk of an opioid-use disorder.
State Marijuana Policy in the Shadow of Potential Federal Enforcement
Overall, the evidence from studies shows promise that marijuana could potentially be useful in alleviating the nation’s growing dependence on opioids, but there is still work that needs to be done. Because the federal government classifies marijuana as a Schedule I controlled substance, there are limits to research on it because obtaining permission to use marijuana in a scientific study is a laborious and time-consuming process that faces many restrictions. For example, little academic research has been done on the potential long-term side effects of marijuana use, which is needed to determine if marijuana is a safe alternative to other medications. Clinical trials where marijuana was prescribed rather than opioids would provide valuable information. Marijuana research is caught in something of a chicken or the egg paradox — marijuana is labeled a Schedule I drug partially because it has been deemed to have “no medical use,” but marijuana cannot easily be studied for medical use because it is a Schedule I drug.
While Attorney General Jeff Sessions has dismissed any evidence that medical marijuana reduces opioid use and deaths, he did concede in a recent hearing of the Senate Committee on Appropriations Subcommittee on Commerce, Justice, Science, and Related Agencies that there “may well be some benefits from medical marijuana.” Sessions also indicated that the federal government was planning to take steps to allow more licenses to grow marijuana for research.
A new bill recently introduced by a bipartisan coalition in the House of Representatives would go further; the Medical Cannabis Research Act of 2018 would provide “safe harbor” for federally supported institutions that want to conduct research on marijuana, but have been hesitant to do so as to not jeopardize their funding. The legislation would also permit healthcare providers at Veterans Affairs to provide information to patients about federally approved marijuana clinical trials. The Medical Cannabis Research Act of 2018 would not change the status of marijuana as a Schedule I drug or impact its legalization in states.
Until we learn more, it is hard to know if marijuana is a potential alternative to, or deterrent of, opioid use. Research to this point has been encouraging, but it has been limited by the current prohibitions on the use of marijuana in scientific studies. Opioid-related deaths continue to climb, providing a potential impetus for federal lawmakers to reconsider some of the restraints currently placed on marijuana research in search of a way to stem the tide of the epidemic.
Heather Trela is chief of staff and a fellow at the Rockefeller Institute of Government.